Associations between Blood Metabolic Profile at 7 Years Old and Eating Disorders in Adolescence: Findings from the Avon Longitudinal Study of Parents and Children

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Descriptives
2.2. Metabolic Markers Associated with Anorexia Nervosa
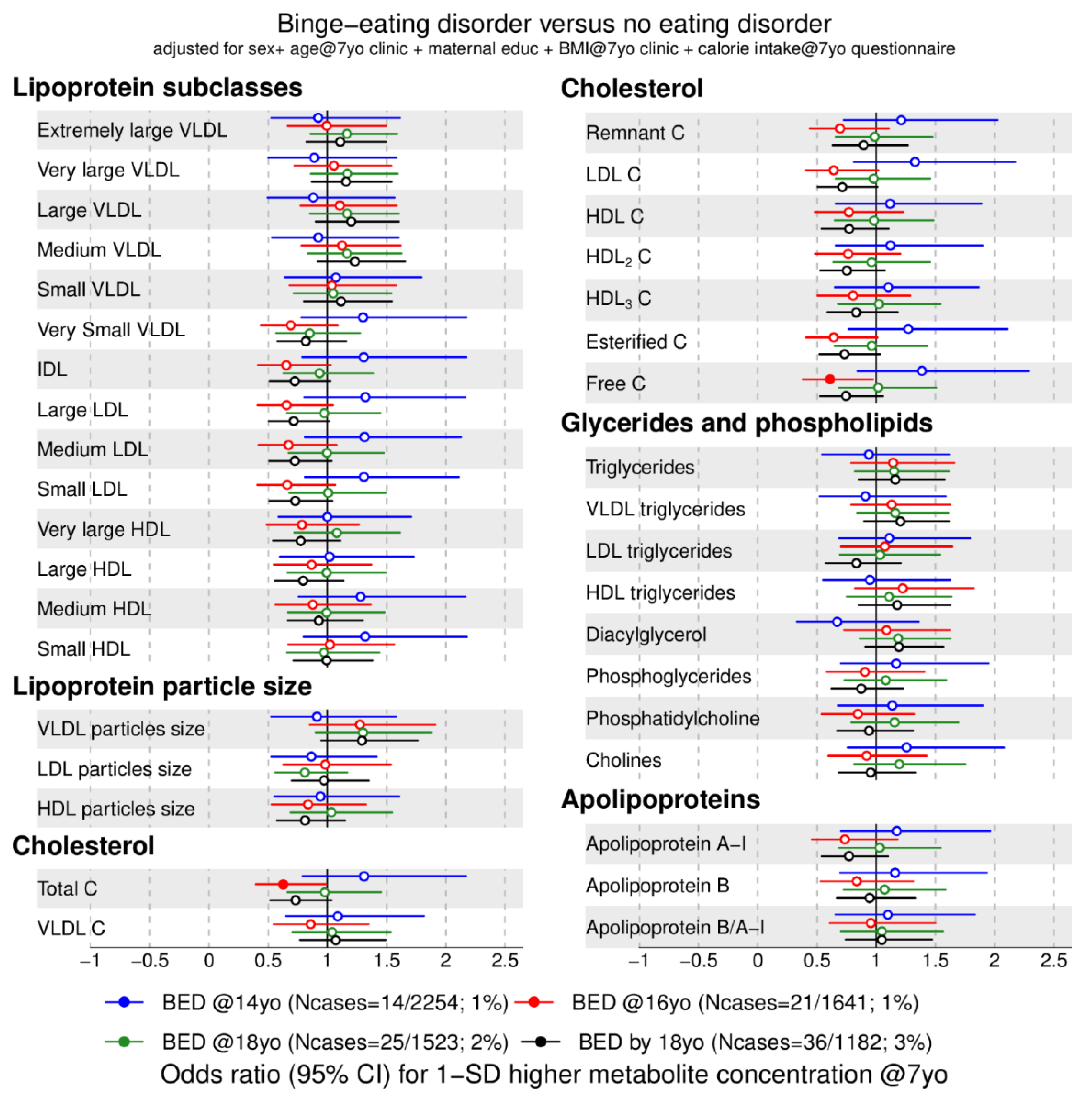
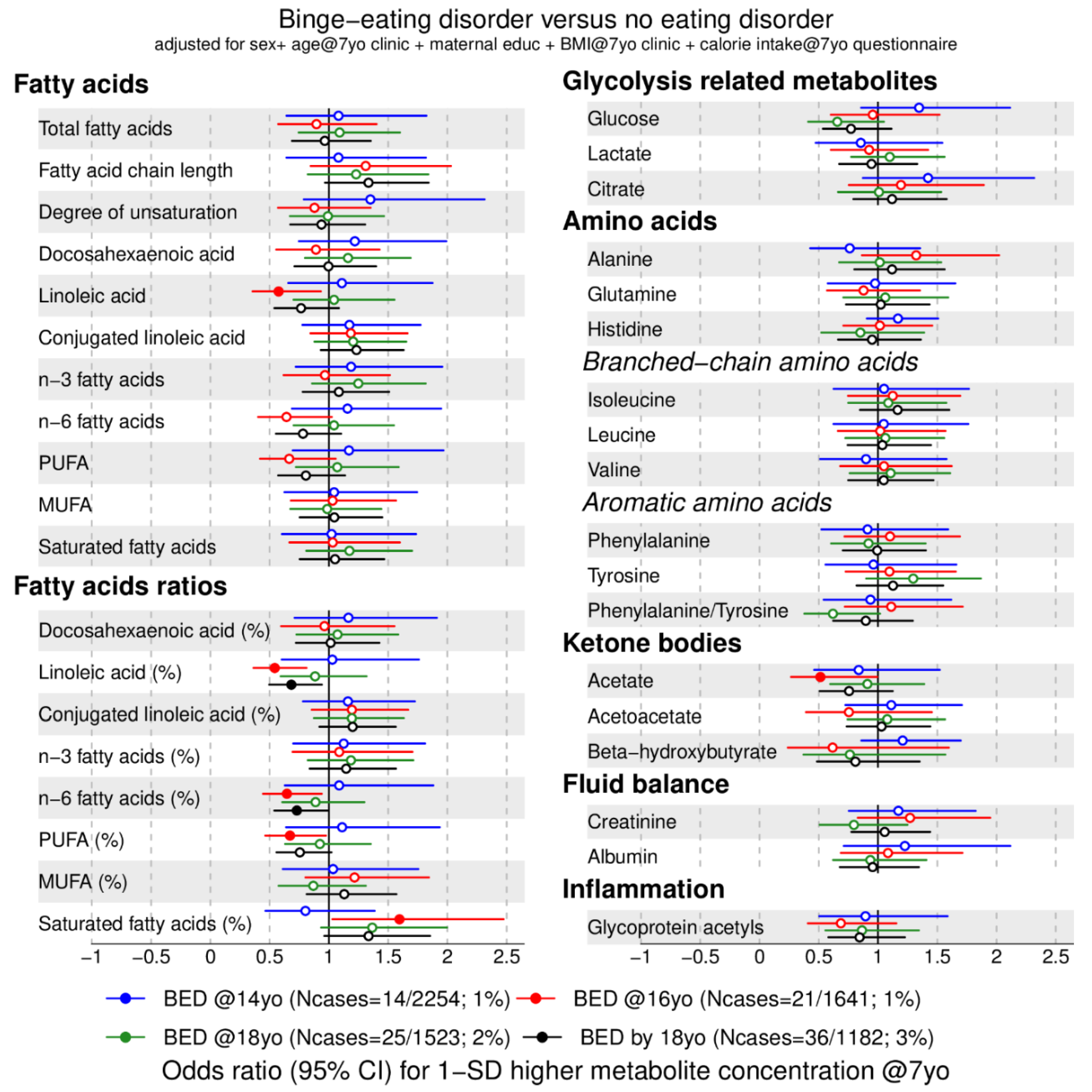
2.3. Metabolic Markers Associated with Binge-Eating Disorder
2.4. Sensitivity Analyses
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Eating Disorders Diagnoses and Covariates
4.3. EDTA-Plasma Metabolome Profiling
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Lipoprotein Subclasses and Fatty Acids Details
References
- Berkman, N.D.; Lohr, K.N.; Bulik, C.M. Outcomes of eating disorders: A systematic review of the literature. Int. J. Eat. Disord. 2007, 40, 293–309. [Google Scholar] [CrossRef] [PubMed]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders A meta-analysis of 36 Studies. Arch Gen. Psychiat. 2011, 68, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Culbert, K.M.; Racine, S.E.; Klump, K.L. Research Review: What we have learned about the causes of eating disorders—A synthesis of sociocultural, psychological, and biological research. J. Child Psychol. Psychiatry 2015, 56, 1141–1164. [Google Scholar] [CrossRef] [PubMed]
- Eating Disorders Working Group of the Psychiatric Genomics Consortium; Duncan, L.; Yilmaz, Z.; Gaspar, H.; Walters, R.; Goldstein, J.; Anttila, V.; Bulik-Sullivan, B.; Ripke, S.; Thornton, L.; et al. Significant locus and metabolic genetic correlations revealed in genome-wide association study of anorexia nervosa. Am. J. Psychiatry 2017, 174, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Eating Disorders Working Group of the Psychiatric Genomics Consortium (PGC-ED); Watson, H.J.; Yilmaz, Z.; Thornton, L.M.; Hübel, C.; Coleman, J.R.I.; Gaspar, H.A.; Wade, T.D.; Birgegård, A.; Lichtenstein, P.; et al. Anorexia nervosa genome-wide association study identifies eight loci and implicates metabo-psychiatric origins. Nat. Genet. 2019, 51, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, A.; Hübel, C.; Stahl, D.; Stadler, M.; Ismail, K.; Breen, G.; Treasure, J.; Kan, C. The metabolic underpinning of eating disorders: A systematic review and meta-analysis of insulin sensitivity. Mol. Cell. Endocrinol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Focker, M.; Timmesfeld, N.; Scherag, S.; Knoll, N.; Singmann, P.; Wang-Sattler, R.; Buhren, K.; Schwarte, R.; Egberts, K.; Fleischhaker, C.; et al. Comparison of metabolic profiles of acutely ill and short-term weight recovered patients with anorexia nervosa reveals alterations of 33 out of 163 metabolites. J. Psychiatr. Res. 2012, 46, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Da Luz, F.Q.; Hay, P.; Touyz, S.; Sainsbury, A. Obesity with comorbid eating disorders: Associated health risks and treatment approaches. Nutrients 2018, 10, 829. [Google Scholar] [CrossRef] [PubMed]
- Abraham, T.M.; Massaro, J.M.; Hoffmann, U.; Yanovski, J.A.; Fox, C.S. Metabolic Characterization of adults with binge eating in the general population: The Framingham Heart Study. Obesity 2014, 22, 2441–2449. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Guo, J.; Story, M.; Haines, J.; Eisenberg, M. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: How do dieters fare 5 years later? J. Am. Diet. Assoc. 2006, 106, 559–568. [Google Scholar] [CrossRef]
- Herle, M.; Stavola, B.; Hubel, C.; Abdulkadir, M.; Ferreira, D.S.; Loos, R.J.F.; Bryant-Waugh, R.; Bulik, C.M.; Micali, N. A longitudinal study of eating behaviours in childhood and later eating disorder behaviours and diagnoses. Br. J. Psychiatry 2019. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Z.; Gottfredson, N.C.; Zerwas, S.C.; Bulik, C.M.; Micali, N. Developmental premorbid body mass index trajectories of adolescents with eating disorders in a longitudinal population cohort. J. Am. Acad. Child Psychiatry 2019, 58, 191–199. [Google Scholar] [CrossRef]
- Hussain, A.A.; Hubel, C.; Hindborg, M.; Lindkvist, E.; Kastrup, A.M.; Yilmaz, Z.; Stoving, R.K.; Bulik, C.M.; Sjogren, J.M. Increased lipid and lipoprotein concentrations in anorexia nervosa: A systematic review and meta-analysis. Int. J. Eat. Disord. 2019, 52, 611–629. [Google Scholar] [CrossRef]
- Weinbrenner, T.; Zuger, M.; Jacoby, G.E.; Herpertz, S.; Liedtke, R.; Sudhop, T.; Gouni-Berthold, I.; Axelson, M.; Berthold, H.K. Lipoprotein metabolism in patients with anorexia nervosa: A case-control study investigating the mechanisms leading to hypercholesterolaemia. Br. J. Nutr. 2004, 91, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Micali, N.; Field, A.E.; Treasure, J.L.; Evans, D.M. Are obesity risk genes associated with binge eating in adolescence? Obesity 2015, 23, 1729–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micali, N.; Holliday, J.; Karwautz, A.; Haidvogl, M.; Wagner, G.; Fernandez-Aranda, F.; Badia, A.; Gimenez, L.; Solano, R.; Brecelj-Anderluh, M. Childhood eating and weight in eating disorders: A multi-centre European study of affected women and their unaffected sisters. Psychother. Psychosom. 2007, 76, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Micali, N.; De Stavola, B.; Ploubidis, G.; Simonoff, E.; Treasure, J.; Field, A.E. Adolescent eating disorder behaviours and cognitions: Gender-specific effects of child, maternal and family risk factors. Br. J. Psychiatry 2015, 207, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A.E.; Sonneville, K.R.; Micali, N.; Crosby, R.D.; Swanson, S.A.; Laird, N.M.; Treasure, J.; Solmi, F.; Horton, N.J. Prospective association of common eating disorders and adverse outcomes. Pediatrics 2012, 130, E289–E295. [Google Scholar] [CrossRef]
- Micali, N.; Solmi, F.; Horton, N.J.; Crosby, R.D.; Eddy, K.T.; Calzo, J.P.; Sonneville, K.R.; Swanson, S.A.; Field, A.E. Adolescent eating disorders predict psychiatric, high-Risk behaviors and weight outcomes in young adulthood. J. Am. Acad. Child Psychiatry 2015, 54, 652–659. [Google Scholar] [CrossRef]
- Baskaran, C.; Eddy, K.T.; Miller, K.K.; Meenaghan, E.; Misra, M.; Lawson, E.A. Leptin secretory dynamics and associated disordered eating psychopathology across the weight spectrum. Eur. J. Endocrinol. 2016, 174, 503–512. [Google Scholar] [CrossRef] [Green Version]
- Pinto, J.; Domingues, M.R.; Galhano, E.; Pita, C.; Almeida Mdo, C.; Carreira, I.M.; Gil, A.M. Human plasma stability during handling and storage: Impact on NMR metabolomics. Analyst 2014, 139, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Mall, C.; Taylor, S.L.; Hitchcock, S.; Zhang, C.; Wettersten, H.I.; Jones, A.D.; Chapman, A.; Weiss, R.H. Mealtime, temporal, and daily variability of the human urinary and plasma metabolomes in a tightly controlled environment. PLoS ONE 2014, 9, e86223. [Google Scholar] [CrossRef] [PubMed]
- Carayol, M.; Licaj, I.; Achaintre, D.; Sacerdote, C.; Vineis, P.; Key, T.J.; Moret, N.C.O.; Scalbert, A.; Rinaldi, S.; Ferrari, P. Reliability of serum metabolites over a two-year period: A targeted metabolomic approach in fasting and non-fasting samples from EPIC. PLoS ONE 2015, 10, e0135437. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.K.; Clish, C.B.; Kraft, P.; Wu, C.; Souza, A.L.; Deik, A.A.; Tworoger, S.S.; Wolpin, B.M. Reproducibility of metabolomic profiles among men and women in 2 large cohort studies. Clin. Chem. 2013, 59, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.K.; Bao, Y.; Poole, E.M.; Bertrand, K.A.; Kraft, P.; Wolpin, B.M.; Clish, C.B.; Tworoger, S.S. Impact of pre-analytic blood sample collection factors on metabolomics. Cancer Epidem. Biomar. 2016, 25, 823–829. [Google Scholar] [CrossRef]
- Dunn, W.B.; Broadhurst, D.I.; Atherton, H.J.; Goodacre, R.; Griffin, J.L. Systems level studies of mammalian metabolomes: The roles of mass spectrometry and nuclear magnetic resonance spectroscopy. Chem. Soc. Rev. 2011, 40, 387–426. [Google Scholar] [CrossRef]
- Fraser, A.; Macdonald-Wallis, C.; Tilling, K.; Boyd, A.; Golding, J.; Davey Smith, G.; Henderson, J.; Macleod, J.; Molloy, L.; Ness, A. Cohort profile: The Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int. J. Epidemiol. 2013, 42, 97–110. [Google Scholar] [CrossRef]
- Boyd, A.; Golding, J.; Macleod, J.; Lawlor, D.A.; Fraser, A.; Henderson, J.; Molloy, L.; Ness, A.; Ring, S.; Davey Smith, G.D. Cohort Profile: The ‘Children of the 90s’-the index offspring of the Avon Longitudinal Study of Parents and Children. Int. J. Epidemiol. 2013, 42, 111–127. [Google Scholar] [CrossRef]
- Emmett, P.M.; Jones, L.R.; Northstone, K. Dietary patterns in the Avon Longitudinal Study of Parents and Children. Nutr. Rev. 2015, 73, 207–230. [Google Scholar] [CrossRef]
- Soininen, P.; Kangas, A.J.; Wurtz, P.; Tukiainen, T.; Tynkkynen, T.; Laatikainen, R.; Jarvelin, M.R.; Kahonen, M.; Lehtimaki, T.; Viikari, J.; et al. High-throughput serum NMR metabonomics for cost-effective holistic studies on systemic metabolism. Analyst 2009, 134, 1781–1785. [Google Scholar] [CrossRef]
- Wurtz, P.; Kangas, A.J.; Soininen, P.; Lawlor, D.A.; Davey Smith, G.; Ala-Korpela, M. Quantitative serum nuclear magnetic resonance metabolomics in large-scale epidemiology: A primer on -omic technologies. Am. J. Epidemiol. 2017, 186, 1084–1096. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Ferreira, D.L.S.; Nelson, S.M.; Sattar, N.; Ala-Korpela, M.; Lawlor, D.A. Metabolic characterization of menopause: Cross-sectional and longitudinal evidence. BMC Med. 2018, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wurtz, P.; Auro, K.; Makinen, V.P.; Kangas, A.J.; Soininen, P.; Tiainen, M.; Tynkkynen, T.; Jokelainen, J.; Santalahti, K.; et al. Metabolic profiling of pregnancy: Cross-sectional and longitudinal evidence. BMC Med. 2016, 14. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, D.L.S.; Williams, D.M.; Kangas, A.J.; Soininen, P.; Ala-Korpela, M.; Smith, G.D.; Jarvelin, M.R.; Lawlor, D.A. Association of pre-pregnancy body mass index with offspring metabolic profile: Analyses of 3 European prospective birth cohorts. PLoS Med. 2017, 14, e1002376. [Google Scholar]
- Santos Ferreira, D.L.; Maple, H.J.; Goodwin, M.; Brand, J.S.; Yip, V.; Min, J.L.; Groom, A.; Lawlor, D.A.; Ring, S. The Effect of pre-analytical conditions on blood metabolomics in epidemiological studies. Metabolites 2019, 9, 64. [Google Scholar] [CrossRef] [PubMed]
- Moyano, D.; Vilaseca, M.A.; Artuch, R.; Lambruschini, N. Plasma amino acids in anorexia nervosa. Eur. J. Clin. Nutr. 1998, 52, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Palova, S.; Charvat, J.; Masopust, J.; Klapkova, E.; Kvapil, M. Changes in the plasma amino acid profile in anorexia nervosa. J. Int. Med. Res. 2007, 35, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Davey Smith, G. Sifting the evidence-what’s wrong with significance tests? Phys. Ther. 2001, 81, 1464–1469. [Google Scholar] [CrossRef]
- Wasserstein, R.L.; Lazar, N.A. The ASA’s Statement on p-Values: Context, Process, and Purpose. Am. Stat. 2016, 70, 129–131. [Google Scholar] [CrossRef]
- Wurtz, P.; Kangas, A.J.; Soininen, P.; Lehtimaki, T.; Kahonen, M.; Viikari, J.S.; Raitakari, O.T.; Jarvelin, M.R.; Davey Smith, G.; Ala-Korpela, M. Lipoprotein subclass profiling reveals pleiotropy in the genetic variants of lipid risk factors for coronary heart disease: A note on Mendelian randomization studies. J. Am. Coll. Cardiol. 2013, 62, 1906–1908. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eating Disorders Status by Assessment Age | n (%) | Female [n (%)] | Age (years) [mean (SD)] | Body Mass Index (kg/m2) [mean (SD)] | Average Total Calorie Intake (kcal) [mean (SD)] | Mother >12 Years in Education [n (%)] |
|---|---|---|---|---|---|---|
| Anorexia Nervosa (N = 2907) | ||||||
| Diagnosis at 14 Years Old | ||||||
| No Eating Disorder | 2224 (96) | 1057 (48)* | 7.5 (0.1) | 15.9 (1.8)* | 1726.3 (304.7)* | 1113 (50) |
| Anorexia Nervosa | 87 (4) | 61 (70)* | 7.5 (0.1) | 14.6 (1.3)* | 1639.4 (255.8)* | 40 (46) |
| Diagnosis at 16 Years Old | ||||||
| No Eating Disorder | 1615 (97) | 729 (45)* | 7.5 (0.1) | 15.7 (1.6)* | 1729.4 (305.0)* | 853 (53) |
| Anorexia Nervosa | 48 (3) | 37 (77)* | 7.4 (0.1) | 14.5 (0.9)* | 1565.8 (261.0)* | 25 (52) |
| Diagosis at 18 Years Old | ||||||
| No Eating Disorder | 1498 (98) | 697 (47)* | 7.4 (0.1) | 15.8 (1.7)* | 1728.9 (304.1) | 814 (54) |
| Anorexia Nervosa | 26 (2) | 21 (81)* | 7.5 (0.1) | 14.6 (1.4)* | 1673.7 (248.9) | 15 (58) |
| Cumulatively Across All Available Time Points (i.e., Eating Disorder Diagnosis at Age 14, 16, or 18 Years Old) | ||||||
| No Eating Disorder | 1146 (90) | 655 (57) | 7.4 (0.1) | 16.1 (1.8)* | 1725.9 (301.6)* | 650 (57) |
| Anorexia Nervosa | 127 (10) | 88 (69) | 7.5 (0.1) | 14.6 (1.2)* | 1636.8 (267.5)* | 63 (50) |
| Binge-Eating Disorder (N = 2879) | ||||||
| Diagnosis at 14 Years Old | ||||||
| No Eating Disorder | 2240 (99) | 1070 (48) | 7.5 (0.1) | 15.9 (1.8) | 1723.3 (304.6) | 1122 (50) |
| Binge-Eating Disorder | 14 (1) | 8 (57) | 7.4 (0.1) | 16.4 (1.1) | 1714.6 (422.2) | 4 (29) |
| Diagnosis at 16 Years Old | ||||||
| No Eating Disorder | 1620 (99) | 732 (45)* | 7.5 (0.1) | 15.7 (1.6)* | 1729.7 (304.5) | 857 (53) |
| Binge-Eating Disorder | 21 (1) | 17 (81)* | 7.4 (0.2) | 16.7 (1.4)* | 1854.9 (263.8) | 10 (48) |
| Diagnosis at 18 Years Old | ||||||
| No Eating Disorder | 1498 (98) | 697 (47)* | 7.4 (0.1) | 15.8 (1.7) | 1728.9 (304.1) | 814 (54) |
| Binge-Eating Disorder | 25 (2) | 20 (80)* | 7.4 (0.1) | 16.8 (1.9) | 1744.1 (329.6) | 15 (60) |
| Cumulatively Across All Available Time Points (i.e., Eating Disorder Diagnosis at Age 14, 16, or 18 Years Old) | ||||||
| No Eating Disorder | 1146 (97) | 655 (57) | 7.4 (0.1) | 16.1 (1.8) | 1725.9 (301.6) | 650 (57) |
| Binge-Eating Disorder | 36 (3) | 27 (75) | 7.4 (0.1) | 16.6 (1.7) | 1808.7 (267.8) | 21 (58) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos Ferreira, D.L.; Hübel, C.; Herle, M.; Abdulkadir, M.; Loos, R.J.F.; Bryant-Waugh, R.; Bulik, C.M.; De Stavola, B.L.; Lawlor, D.A.; Micali, N. Associations between Blood Metabolic Profile at 7 Years Old and Eating Disorders in Adolescence: Findings from the Avon Longitudinal Study of Parents and Children. Metabolites 2019, 9, 191. https://doi.org/10.3390/metabo9090191
Santos Ferreira DL, Hübel C, Herle M, Abdulkadir M, Loos RJF, Bryant-Waugh R, Bulik CM, De Stavola BL, Lawlor DA, Micali N. Associations between Blood Metabolic Profile at 7 Years Old and Eating Disorders in Adolescence: Findings from the Avon Longitudinal Study of Parents and Children. Metabolites. 2019; 9(9):191. https://doi.org/10.3390/metabo9090191
Chicago/Turabian StyleSantos Ferreira, Diana L., Christopher Hübel, Moritz Herle, Mohamed Abdulkadir, Ruth J. F. Loos, Rachel Bryant-Waugh, Cynthia M. Bulik, Bianca L. De Stavola, Deborah A. Lawlor, and Nadia Micali. 2019. "Associations between Blood Metabolic Profile at 7 Years Old and Eating Disorders in Adolescence: Findings from the Avon Longitudinal Study of Parents and Children" Metabolites 9, no. 9: 191. https://doi.org/10.3390/metabo9090191